Corneal Keloid
Authors:
Manusree Bhatter BS*, Christian Robertson MD, Lai Jiang MD
DOI: 10.62856/djcro.v9.63
Introduction
Corneal keloids are relatively rare corneal tumors with benign proliferation of fibrous or fibrovascular tissue in the corneal stroma, hypothesized to originate from the stromal cells of the iris.1,2 Corneal keloids are sometimes confused with hypertrophic scars, but corneal keloids differ by expanding past the area of initial trauma over months and years after the initial insult, compared to hypertrophic scars which appear immediately after trauma and gradually retract with time. Treatment options include keratectomy, lamellar or penetrating keratoplasty, and sclerokeratoplasty.3 Superficial keratectomy is an effective surgical technique to diminish corneal haziness associated with many lesions including corneal keloids.4
Case Report
A 56-year-old male presented with a growth on the left eye that began over the past 2 years developed associated pain and photophobia for the prior 6-8 months. He described the pain as achy and throbbing. He had dryness in both eyes as well, for which he used artificial tears twice daily. The patient noted poor vision in his left eye for several years. He had a past medical history of chronic kidney disease and hypertension. The patient endorsed a history of a left eye injury in childhood with an associated corneal scar.
At initial presentation, best corrected visual acuity was 20/25-2 in the right eye and counting fingers vision in the left eye. The right eye had no remarkable findings on exam. Examination of the left eye revealed a large, elevated, opaque, and smooth corneal lesion extending limbus to limbus in the inferior half of the cornea (Figure 1). The remainder of the exam revealed iris atrophy and scarring in addition to an anterior chamber IOL.
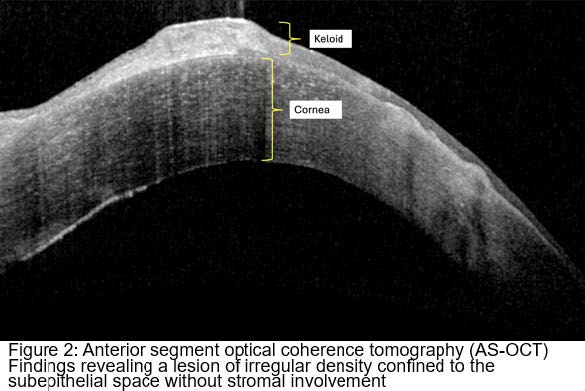
Anterior segment optical coherence tomography (AS-OCT) revealed a lesion of irregular density confined to the subepithelial space without stromal involvement (Figure 2). The corneal mass was removed by superficial keratectomy, and a specimen was sent for pathological evaluation.
Pathology revealed findings consistent with a corneal keloid. One week later, visual acuity in the left eye was 4/200. One month later, visual acuity was 5/200. Underlying deprivation amblyopia following the childhood injury limited visual improvement. Repeat slit lamp photos were taken at this visit (Figure 3).

Pathology findings:
Specimen consisted of a whitish folded piece of tissue measuring 9 x 4.5 x 1.5 mm. Examination revealed cornea with focal thickening of the epithelium, focal thickening of the epithelial basement membrane (PAS stain), and focal pigmentation within the epithelium. Corneal perforation was present near one margin. The stroma was composed of variably dense collagen with focal sclerosis and facets of epithelium within the stroma. Epithelial inclusion cysts were also present within the stroma. Focal keratinization of the epithelium was present. Occasional multinucleated cells were present subjacent to the epithelium. Rare goblet cells were present (PAS stain).
Discussion
Corneal keloids result from the connective tissue response to inflammation, trauma, surgery, or burns. Keloids result from abnormal wound responses that appear as a growing whitish, smooth, and raised single lesion in a previously injured part of the cornea. Generally, corneal keloids are seen within the first 2 decades of life and occur more frequently in males than females. They usually present unilaterally, with bilateral presentation being rare.5 They generally present as localized white elevated lesions varying in thickness and size with slow growth over months to years. They can be congenital or primary lesions but are associated with ocular surface injury and eye surgery, though there have been instances of keloid formation in eyes without corneal injury.6 On pathology, corneal keloids are characterized by hyperplastic epithelium, disorganized basal layer, disrupted Bowman’s layer, and abundant, haphazard arrangement of collagen bundles with activated fibroblasts in the stroma and blood vessels. The underlying cornea can be involved depending on the keloid’s primary pathology.6 They are very similar to hypertrophic scars since hypertrophic scars are also abnormal wound responses. They are both characterized by abundant glycoprotein and collagen deposition but can be distinguished clinically in that keloids extend beyond the original wound and rarely regress. Hypertrophic scars usually regress spontaneously and are raised.5 In earlier stages of the keloid, there is predominant presence of type III collagen, abundant myofibroblasts, and few vessel formations. In later stages of the keloid, we see a predominance of haphazard collagen type I fascicle arrangement and scarce myofibroblasts with blood vessel involution. Immunohistochemical studies of the keloids reveal positive staining for vimentin in active fibroblasts and alphasmooth muscle actin in myofibroblasts.5
Anterior segment imaging is useful in evaluating corneal keloids, especially in cases where there is anterior segment dysgenesis. The AS-OCT revealed an irregular, hyper-reflective lesion confined to the subepithelial space without deep stromal involvement (Figure 2).
Several modalities have been used to treat visually significant corneal keloids depending on the location of the lesion. Superficial keratectomy and phototherapeutic keratectomy are usually the treatment of choice for lesions anterior to Bowman’s layer, while lamellar or penetrating keratoplasty are useful for deeper lesions involving the corneal stroma. There are reported cases of recurrence with superficial keratectomy, lamellar and penetrating keratoplasty, and phototherapeutic keratectomy. Amniotic membrane transplantation has been combined with superficial keratectomy in many cases since amniotic membrane has anti-inflammatory and anti-fibroblastic properties.6 Due to the superficial location of the lesion, we decided that a superficial keratectomy procedure would be best suited for the patient. During the procedure, the lesion was removed using a crescent blade. A Weck-cell sponge was used to remove all residual loose epithelium in the area. The ocular surface was then irrigated with balanced salt solution. One drop of moxifloxacin and prednisolone acetate were placed followed by a bandage contact lens.

Conclusion
This case highlights the diagnostic and therapeutic challenges in managing corneal keloids. A comprehensive approach—including detailed clinical evaluation, AS-OCT imaging, and confirmatory histopathology—is essential for diagnosis. Although our patient had only modest improvement in visual acuity due to deprivation amblyopia, his symptoms resolved after the superficial keratectomy procedure. Further research into adjunctive therapies is warranted to optimize management strategies and enhance patient outcomes.
References
1. Farkas TG, Znajda JP. Keloid of the Cornea. Am J Ophthalmol. 1968;66(2):319-23.
2. Li S, Lei J, Wang YH, et al. Rare Giant Corneal Keloid Presenting 26 Years after Trauma: A Case Report. World J Clin Cases. 2022;10(27):9776-9782
3. Vanathi M, Panda A, Kai S, et al. Corneal Keloid. Ocul Surf. 2008;6(4):186-97.
4. Salari F, Beikmarzehei A, Liu G, et al. Superficial Keratectomy: A Review of Literature. Front Med (Lausanne). 2022;9:915284.
5. Gupta J, Gantyala SP, Kashyap S, et al. Diagnosis, Management, and Histopathological Characteristics of Corneal Keloid: A Case Series and Literature Review. Asia Pac J Ophthalmol (Phila). 2016;5(5):354-9.
6. Lee HK, Choi HJ, Kim MK, et al. Corneal Keloid: Four Case Reports of Clinicopathological Features and Surgical Outcome. BMC Ophthalmol. 2016;16(1):198.
Statement of Ethics
This case series adheres to patient confidentiality and ethical principles in accordance with the guidelines of the Declaration of Helsinki and relevant local regulations.
Conflict of Interest Statement
The authors declare no conflicts of interest related to this topic.
Funding
This work received no funding or grant support.