Dissecting Trabeculectomy Filtering Bleb Masquerading as Ocular Surface Squamous Neoplasia
Authors
Esteban A. Peralta MD*, Arpita S. Maniar MD, Alan D. Proia MD PhD, Syed A. Ahmed, Miguel A. Materin, MD
DOI: 10.62856/djcro.v8.56
Introduction
A 79-year-old woman with glaucoma and a history of trabeculectomy presented with a large conjunctival mass in the right eye that was excised due to concern for ocular surface squamous neoplasia. This case highlights the diagnostic challenge posed by pendulous or keratinized blebs and underscores the importance of histopathologic evaluation in differentiating benign from malignant conjunctival lesions.
Case Report
A 79-year-old female was evaluated by the ocular oncology service for a conjunctival mass in the right eye accompanied by persistent tearing and impaired central vision. The atypical conjunctival lesion was noted several months earlier and was enlarging with the development of vascularization, prompting referral. The patient had primary open angle glaucoma for which she underwent trabeculectomy in both eyes two years prior. Best corrected visual acuity was 20/400 in the right eye and 20/50 in the left eye, and the IOP was 19 mmHg in the right eye and 20 mmHg in the left eye.
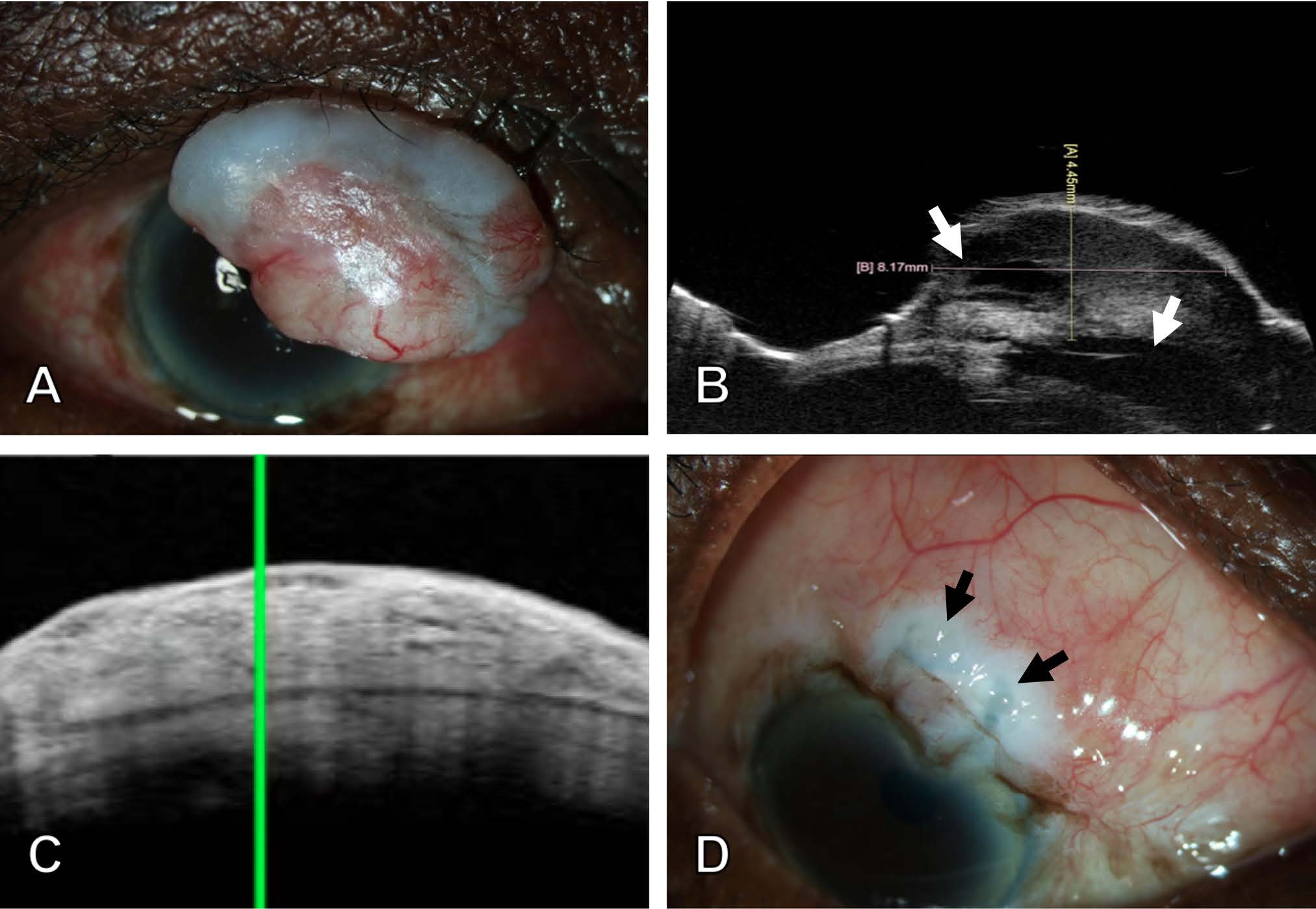
Anterior segment examination of the right eye showed an elevated conjunctival lesion measuring approximately 13 mm x 8 mm arising from the superior bulbar conjunctiva and was overhanging the cornea without any apparent corneal invasion (Figure 1A). There were intrinsic vessels and vessels feeding the lesion, raising suspicion for malignancy. Ultrasound biomicroscopy demonstrated an encapsulated mass with thickened hyperreflective epithelium, heterogeneous echogenicity, and a height of 4.5 mm (Figures 1B-C). The left eye had a superior filtering bleb in the same location. The bleb in the right eye was not visible, but it was presumed to be beneath the amelanotic mass.
The patient underwent an excisional biopsy with an amniotic membrane graft due to the concern for squamous cell carcinoma. Intraoperatively, the lesion was dissected off the cornea in a clear plane and sent to pathology. About six weeks postoperatively, the underlying filtering bleb was functioning (Figure 1D), and visual acuity improved to 20/20 and the IOP was 13 mmHg.
Microscopic examination was performed on sections representing the entire mass. The mass had a histological appearance typical of an accessory glaucoma filtering bleb.1-4 Stratified squamous epithelium had basal hydropic change with focal thickening and keratinization, most likely due to tear-film breakup. No dysplasia or carcinoma was identified. The subepithelial stroma had areas of dense fibrovascular tissue with increased vascularity and telangiectasia, typical of a multiloculated filtering bleb (Figures 2A-B).1,4 Much of the stroma was expanded by edema. Subepithelial areas of bright eosinophilia (Figure 2C) had the tinctorial property of dense collagen using a Masson trichrome stain (Figure 2D). This subepithelial hypocellular zone of collagen was reported in a failed bleb after mitomycin C therapy5 but is a common feature of encapsulated glaucoma blebs in our experience.

Discussion
This case highlights the potential for glaucoma filtering blebs to become pendulous, overhang the cornea, and then undergo atypical epithelial keratinization, simulating ocular surface squamous neoplasia. While postoperative complications of glaucoma filtering blebs most commonly include leakage, infection, or overfiltration, this case highlights an unusual presentation of a benign conjunctival mass arising from an accessory bleb following trabeculectomy surgery.
Histopathological examination was crucial in ruling out malignancy and confirming the diagnosis of a loculated accessory filtering bleb. The presence of keratinized epithelium, subepithelial edema, and hypocellular zones of dense collagen correlated with features described in dissecting glaucoma blebs treated with adjunctive mitomycin C.1,4,5 This reinforces the importance of biopsy in ambiguous conjunctival lesions, particularly in eyes that have had prior ophthalmic surgery.
Conclusion
Clinicians should consider this rare diagnosis in the differential when encountering conjunctival masses in glaucoma patients with a history of trabeculectomy or any prior eye surgery. Early recognition and appropriate management, as demonstrated here, can result in excellent functional outcomes with preserved vision and IOP. Further studies on long-term outcomes of such cases may help refine diagnostic and treatment protocols.
References
1. Teng C, Chi H, Katzin H. Histology and Mechanism of Filtering Operations. Am. J. Ophthalmol. 1959;47:16-34.
2. Addicks EM, Quigley HA, Green WR, et al. Histologic Characteristics of Filtering Blebs in Glaucomatous Eyes. Arch. Ophthalmol. 1983;101:795-798.
3. Hutchinson AK, Grossniklaus HE, Brown RH, et al. Clinicopathologic Features of Excised Mitomycin Filtering Blebs. Arch. Ophthalmol. 1994;112:74-79.
4. Ulrich GG, Proia AD, Shields MB. Clinicopathologic Features and Surgical Management of Dissecting Glaucoma Filtering Blebs. Ophthalmic Surg. 1997;28:151-155.
5. Shields MB, Scroggs MW, Sloop CM, et al. Clinical and Histopathologic Observations Concerning Hypotony after Trabeculectomy with Adjunctive Mitomycin C. Am. J. Ophthalmol. 1993;116(6):673-83.
Statement of Ethics
This case report adheres to patient confidentiality and ethical principles in accordance with the guidelines of the Declaration of Helsinki and relevant local regulations. Consent was obtained from the patient for the publication of this case report.
Conflict of Interest Statement
The authors declare no conflicts of interest related to this topic.
Funding
This work received no funding or grant support.
Authorship
We attest that all authors contributed significantly to the creation of this manuscript, each having fulfilled the criteria as established by the ICMJE.