HLA-B27 positive juvenile idiopathic arthritis associated uveitis presenting with an acute onset and a chronic course
Author
Arash Maleki MD*
DOI: 10.62856/djcro.v8.49
Introduction
Juvenile idiopathic arthritis (JIA) is a chronic rheumatological condition of unknown origin, characterized by arthritis lasting more than six weeks in children and adolescents under the age of 16.1 Uveitis is the most prevalent extra-articular manifestation observed in JIA.2 The reported incidence of uveitis in JIA varies significantly across studies, but the point prevalence is frequently documented as ranging between 10-15%.2
Currently, human leukocyte antigen B27 (HLA-B27) plays a central role in the classification of JIA and serves as an inclusion criterion for the enthesitis-related arthritis category. The presence of HLA-B27 has been shown to predict a more prolonged disease course and is associated with greater age at disease onset in male patients.3 Thus far, bilateral granulomatous panuveitis has not been documented in the literature in association with HLA-B27 JIA.
This case details the occurrence of HLA-B27-associated bilateral granulomatous panuveitis in a 10-year-old female who was ultimately diagnosed with oligoarticular JIA.
Case Report
A 10-year-old girl was evaluated for redness, pain, and photophobia in both eyes, particularly in the left eye. The symptoms had begun two weeks before presentation. Erythromycin ointment had been administered at the onset of symptoms, but this was later switched to ofloxacin drops, leading to a slight improvement in the right eye. There were no photopsias, floaters, headaches, recent flu-like symptoms, systemic illnesses, or skin, joint, or hearing problems. Best-corrected visual acuity (BCVA) was 20/20 in the right eye and 20/40 in the left eye. Intraocular pressure (IOP) was 21 mmHg in the right eye and 19 mmHg in the left eye. Slit-lamp examination revealed mild conjunctival injection in both eyes; mutton-fat and fine keratic precipitates in both eyes in Arlt's triangle; anterior chamber reaction with 1+ cells in the right and 4+ cells in the left eyes, and 2+ cells in the anterior vitreous of both eyes. Dilated ophthalmoscopy revealed no vitreous haze in the right eye and 1+ vitreous haze in the left eye. The rest of the exam was normal (Figures 1a, b).

f. Two months after starting golimumab infusions, both eyes appear normal.
At presentation, optical coherence tomography (OCT) of the macula showed normal structure and contour in both eyes without significant choroidal thickening. OCT of the optic nerve demonstrated slight retinal nerve fiber layer thickening in the left eye. Fluorescein angiography (FA) showed mild peripheral retinal vascular leakage in both eyes and mild disc leakage and staining in the left eye (Figures 2a, b). Indocyanine green (ICG) angiography revealed hypocyanescent lesions in the choroid in both eyes, mostly in the temporal choroid, suggesting active choroiditis in both eyes (Figures 3a, b).
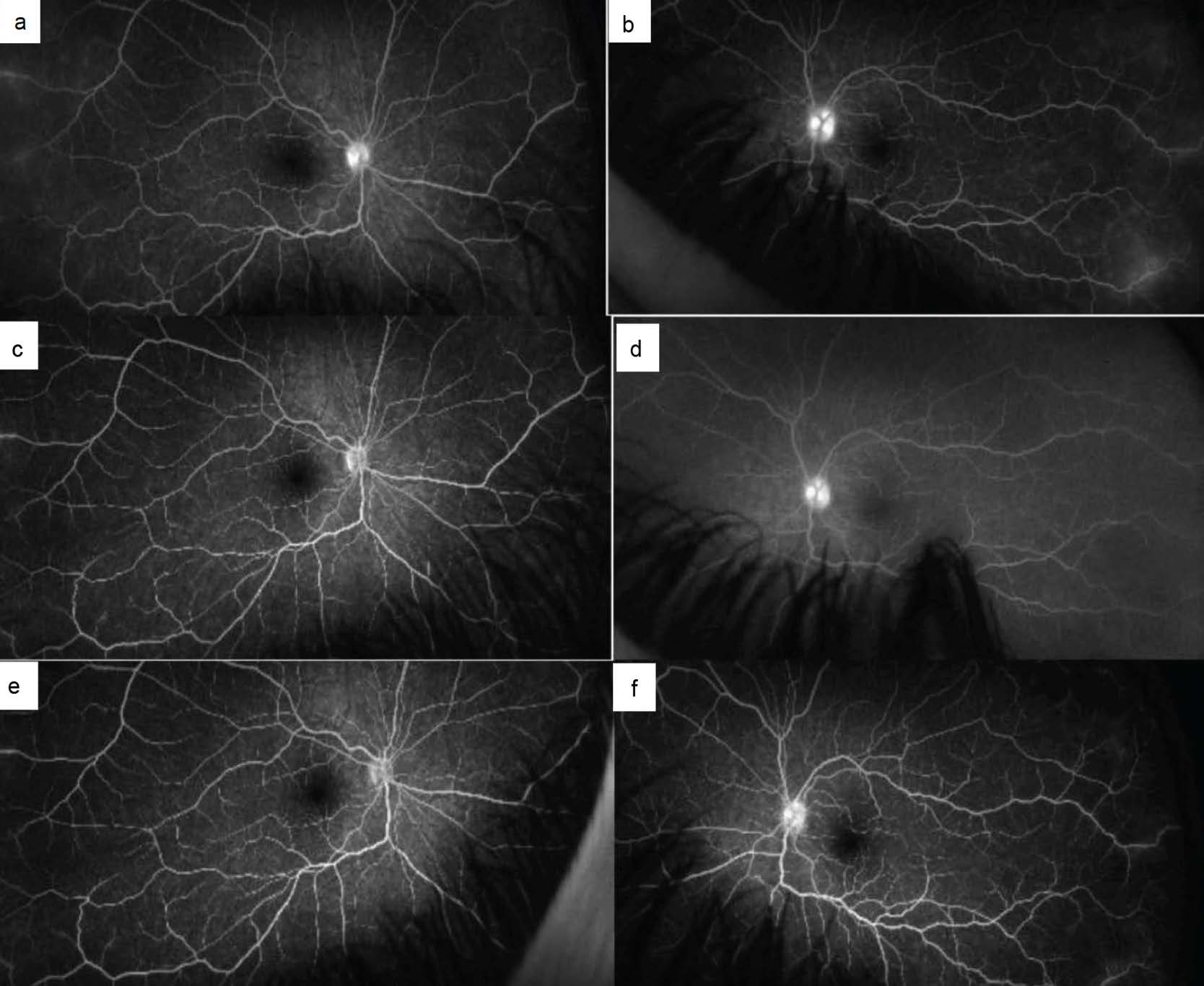
the resolution of disc and vascular leakage and staining in the right eye and improvement in the left. e, f. Two months after starting golimumab infusions, FA at 5 minutes demonstrated that the optic disc leakage
and staining resolved in the right eye and continued to improve in the left eye.
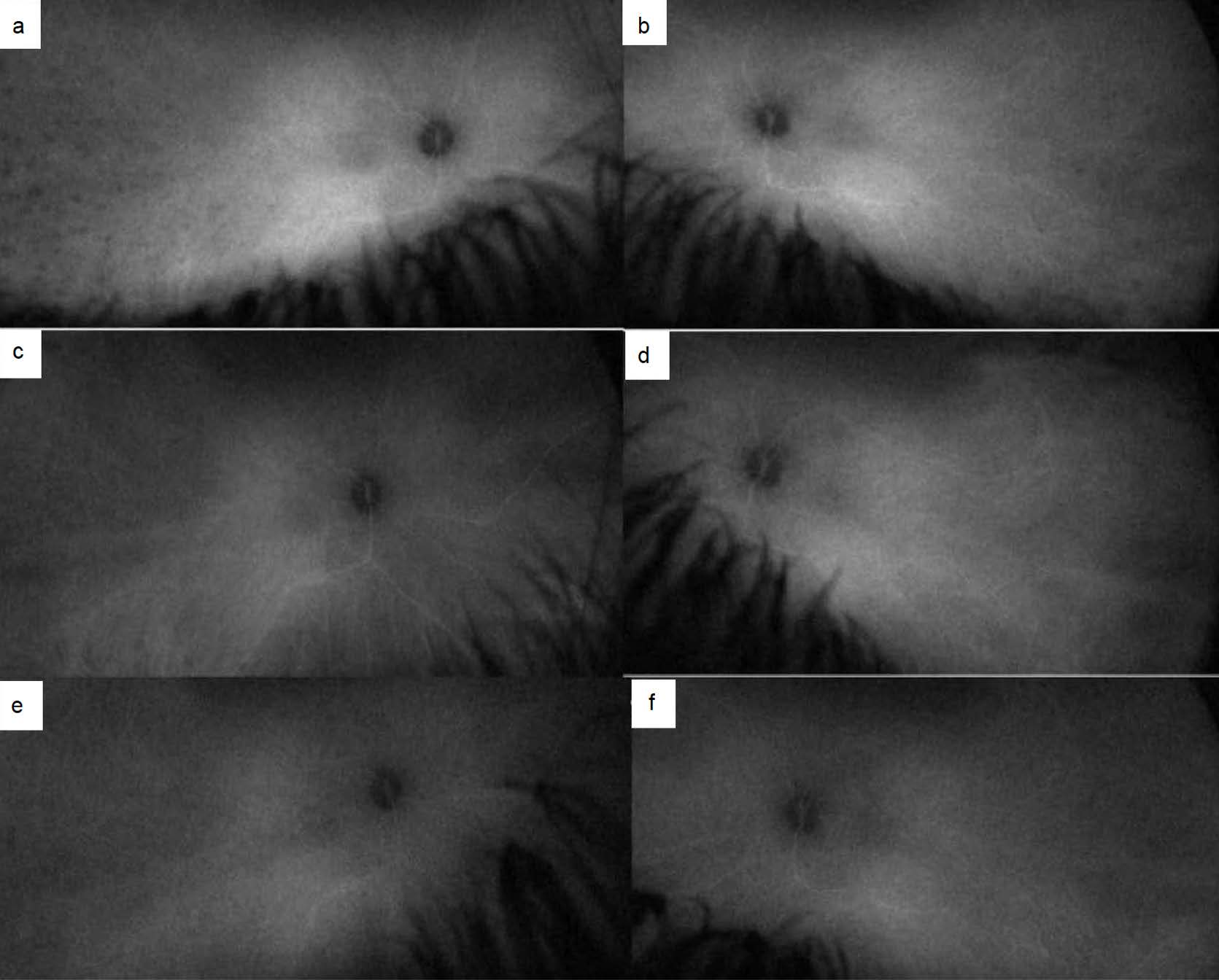
vasculitis in either eye. c, d. One month later, ICG depicted improved choroiditis in both eyes. e, f. Two months after starting golimumab infusions, ICG at 15 minutes demonstrated that the choroiditis remained
markedly improved without evidence of choroidal vasculitis in either eye.
A comprehensive blood workup including complete blood count, erythrocyte sedimentation rate, C-reactive protein, antinuclear antibody, anti-neutrophil cytoplasmic antibody, urinalysis, interleukin 6 (IL-6), human leukocyte antigen B27 (HLA-B27), B44, B51, DR1, DR4, DR15, angiotensin converting enzyme (ACE), lysozyme, 25-hydroxy vitamin D, 1,25-dihydroxy vitamin D, Quantiferon-TB gold, rapid plasma reagin, Lyme Western blot, and Treponema pallidum-particle agglutination were within the normal limits or negative; however, HLA-B27 was positive. A pediatric rheumatology consultation was unremarkable. A chest CT scan team was normal, without lung involvement or hilar lymphadenopathy. Given the diagnosis of panuveitis and Harada-like disease, 40 mg of prednisone (1 mg/kg), atropine 1% twice daily, and prednisolone acetate 1% every two hours with a slow tapering schedule were initiated.
One week later, there was improvement. The prednisolone was placed on a weekly tapering schedule, and the oral prednisone was tapered by 5 mg every two weeks. One month later, BCVA was 20/20 in both eyes and IOP 20 mmHg in both eyes. The anterior and posterior segment examinations (Figures 1c, d), OCT macula and optic nerve, FA (Figures 2c, d), and ICG (Figures 3c, d) were markedly improved. The eyes remained quiet until a recurrence developed, marked by 2+ AC reaction in both eyes and 1+ vitreous haze in the left eye, despite the patient being on a regimen of 10 mg oral prednisolone and twice daily topical prednisolone in both eyes. At this point, immunomodulatory therapy (IMT) was initiated, and adalimumab was started at a dose of 40 mg biweekly, including two loading doses, along with orally administered methotrexate at a dose of 15 mg weekly. Corticosteroid therapy remained unchanged for a month before gradually tapering off entirely within the following month.
The eyes remained in remission on this regimen for nine months. At that time, she developed arthritis in the left knee and left wrist, along with bilateral sacroiliitis confirmed by ultrasound and magnetic resonance imaging (MRI). Given the ineffectiveness of adalimumab and the superior efficacy of golimumab on the joints, the pediatric rheumatology team opted to transition to golimumab therapy while increasing the dose of subcutaneous methotrexate to 20 mg. Two months later, eye examination revealed remission (Figures 1e, f) exams with improved joint signs and symptoms. OCT macula and optic nerve, FA (Figures 2e, f), and ICG (Figures 3e, f) remained markedly improved.
Discussion
JIA-associated uveitis is recognized for its challenging prognosis and high risk of complications. The condition has significant consequences for patients and their families. Timely diagnosis and treatment are paramount for a favorable long-term prognosis.4 Uveitis associated with JIA typically manifests as chronic, non-granulomatous anterior uveitis. The uveitis can be the first manifestation of JIA in 3%–7% of patients and may initially be asymptomatic.4
Juvenile seronegative spondyloarthropathy (JSpA) is a subtype of JIA associated with uveitis. It encompasses conditions such as psoriatic arthritis, ankylosing spondylitis, enthesitis-related arthritis, reactive arthritis, and enteropathic arthritis. Two cohorts of JSpA showed that enthesitis-related arthritis had a high rate of HLA-B27 positivity.5 The arthritis typically exhibits asymmetry and oligoarticularity, and it predominantly affects larger joints in the lower extremities. Hip arthritis supports the diagnosis, and axial involvement has been documented in up to 30% of children within 15 months of diagnosis.6 Acute anterior uveitis is one of the extra-articular manifestations of JSpA. Uveitis is characterized by sudden unilateral inflammation accompanied by redness, pain, and photophobia. It is observed in approximately one-quarter of children with JSpA7; however, uveitis can be asymptomatic.8
This case report is unique because JIA-associated uveitis is typically bilateral, asymptomatic, and chronic or presents with a unilateral acute onset that recurs over time. However, this patient exhibited an unusual presentation, with a bilateral acute onset that progressed to a chronic course, as she remained dependent on topical and oral corticosteroids until the initiation of IMT.
Zuber and colleagues9 diagnosed uveitis in 5.6% of their patients, mainly in those with oligoarthritic arthritis and enthesis-related arthritis. Among such children, 64.3% tested positive for the HLA-B27 antigen. The median age of onset of JIA in these individuals was 13.5 years. Heiligenhaus and colleagues10 reported that acute symptomatic uveitis alternated between two eyes in 20% of patients with enthesitis-related JIA. Ryptal et al.3 documented intermediate uveitis and panuveitis in one (1.4%) and two (2.8%) of their patients, respectively. In their study, six out of nine patients with an acute course of uveitis were positive for HLAB27, and among those, five exhibited HLA positive enthesitis-related arthritis. Although these studies offer invaluable insights into the characteristics of HLA-B27 positive patients with JIA and JIA-associated uveitis, they lack details on the uveitis itself.
We excluded sarcoidosis as a diagnosis for our patient, as all relevant blood tests—including ACE, lysozyme, 25-hydroxy vitamin D, and 1,25-hydroxy vitamin D—were negative. Furthermore, a chest CT scan showed no abnormalities, and as the course progressed, the patient met the criteria for JIA along with its associated uveitis, arthritis in one or more joints persisting for at least six weeks, commencing prior to the age of 16, and notably accentuated by her HLA-B27 positivity.
Our case is unique: both axial and peripheral joints were involved without any signs of enthesitis.9,10 The combination of bilateral, granulomatous uveitis with acute onset and a chronic course has not been previously reported in HLA-B27 positive JIA-associated uveitis. Indocyanine green angiography was instrumental in confirming choroidal involvement, revealing multiple hypofluorescent lesions indicative of active choroiditis.
Considering the extensive eye involvement in our patient, it may be justifiable to conduct more comprehensive evaluations of the retina and choroid using multimodal imaging in patients with HLA-B27 JIA-associated uveitis. Moreover, the fact that our patient responded to the initial immunomodulatory therapy but later showed the involvement of axial and extra-axial joints suggests the need for a more thorough evaluation of the joints using advanced techniques such as ultrasound and MRI for the large peripheral and axial joints. The aim of this proactive approach would be to detect joint involvement before symptoms manifest in HLA-B27 positive patients with uveitis. These considerations seem crucial, as extensive eye involvement and possible systemic involvement may necessitate earlier initiation of IMT with more potent agents, and thus delay systemic involvement in cases of isolated, limited eye findings. However, these hypotheses should be verified with more studies.
We acknowledge that there may be criticism for not initiating IMT promptly after diagnosing our patient with bilateral panuveitis featuring a granulomatous anterior uveitis component and a possible Vogt-Koyanagi-Harada (VKH) diagnosis. However, we note the following considerations. First, our comprehensive lab workup revealed no abnormalities except for a positive HLA-B27 antigen. Pediatric rheumatology consultation to assess for extraocular active and inactive signs of HLA-B27 positivity yielded negative results. Second, the patient exhibited no other symptoms or signs indicative of VKH and had no recent history of flu-like illness. As such, the diagnosis of Harada-like disease was made. Recognizing the requirement for long-term, aggressive IMT in cases of VKH or Harada disease, we initiated treatment with oral corticosteroids and implemented a gradual taper before deciding to use IMT, especially since her family was not prepared for long-term IMT therapy or aggressive procedures such as lumbar puncture for the evaluation of cerebrospinal fluid.
Conclusion
Bilateral panuveitis with a granulomatous anterior uveitis component, characterized by an acute onset and chronic course, coupled with a delayed-onset of oligoarticular JIA involving both axial and extra-axial components, may indicate HLA-B27-associated JIA. The significance of this case lies in the distinctive presentation, which underscores the need for thorough systemic and ophthalmic investigations in similar patients.
References
1. Petty RE, Southwood TR, Manners P, et al. International League of Associations for Rheumatology. International League of Associations for Rheumatology Classification of Juvenile Idiopathic Arthritis: Second Revision, Edmonton, 2001. J Rheumatol. 2004;31(2):390-2.
2. Rypdal V, Glerup M, Songstad NT, et al. Nordic Study Group of Pediatric Rheumatology. Uveitis in Juvenile Idiopathic Arthritis: 18-Year Outcome in the Population-based Nordic Cohort Study. Ophthalmology. 2021;128(4):598-608.
3. Berntson L, Nordal E, Aalto K, et al. Nordic Study Group of Paediatric Rheumatology. HLA-B27 Predicts A More Chronic Disease Course in an 8-year Followup Cohort of Patients with Juvenile Idiopathic Arthritis. J Rheumatol. 2013;40(5):725-31.
4. Heiligenhaus A, Heinz C, Edelsten C, et al. Review for Disease of the Year: Epidemiology of Juvenile Idiopathic Arthritis and its Associated Uveitis: The Probable Risk Factors. Ocul Immunol Inflamm. 2013;21(3):180-91.
5. Weiß A, Minden K, Listing J, et al. Course of Patients with Juvenile Spondyloarthritis During 4 Years of Observation, Juvenile Part of GESPIC. RMD Open. 2017;3(1):e000366. Weiss PF, Klink AJ, Behrens EM, et al. Enthesitis in an Inception Cohort of Enthesitis-related Arthritis. Arthritis Care Res (Hoboken). 2011;63(9):1307-12.
6. Pagnini I, Savelli S, Matucci-Cerinic M, et al. Early Predictors of Juvenile Sacroiliitis in Enthesitisrelated Arthritis. J Rheumatol. 2010;37(11):2395-401.
7. Zeboulon N, Dougados M, Gossec L. Prevalence and Characteristics of Uveitis in the Spondyloarthropathies: A Systematic Literature Review. Ann Rheum Dis. 2008;67(7):955-9.
8. Rychwalski PJ, Cruz OA, Alanis-Lambreton G, et al. Asymptomatic Uveitis in Young People with Inflammatory Bowel Disease. J AAPOS. 1997;1(2):111-14.
9. Żuber Z, Turowska-Heydel D, Sobczyk M, et al. Prevalence of HLA-B27 Antigen in Patients with Juvenile Idiopathic Arthritis. Reumatologia. 2015;53(3):125-30.
10. Heiligenhaus A, Minden K, Föll D, et al. Uveitis in Juvenile Idiopathic Arthritis. Dtsch Arztebl Int. 2015;112(6):92-100.
Statement of Ethics
This case report adheres to patient confidentiality and ethical principles in accordance with the guidelines of the Declaration of Helsinki and relevant local regulations. A written informed consent was obtained from the patient’s parents authorizing publication of this medical case and accompanying images.
Conflict of Interest Statement
The author declares no conflicts of interest related to this topic.
Funding
This work received no funding or grant support.
Authorship
Arash Maleki’s contribution to this study included the conception and design, data analysis and interpretation, drafting of the manuscript, and approval of the final version.