Multimodal Imaging of Punctate Outer Retinal Toxoplasmosis
Authors
Rachel A. Donaldson BS, Aaron Lindeke-Myers MD, Daniel Apple MD, Ramiro S. Maldonado MD*
Introduction
Ocular toxoplasmosis is an intracellular infection caused by the protozoan Toxoplasmosa gondii, with ~2% of infected individuals affected by ocular disease.1 Presentation can be systemic or limited to the eye, even causing necrotizing retinitis. Congenital disease or immunocompromised status increases the risk of severe presentation.2 Symptomatic cases typically present with floaters and/or vision loss. Diagnosis is based on the dilated ophthalmic examination plus serologic and/or polymerase chain reaction testing of intraocular fluid samples. However, the diagnosis can be challenging given the high incidence of seropositive individuals and variable sensitivity of aqueous humor samples.
Typical examination findings include white focal retinitis with vitreous inflammation (“headlight in the fog”) and a pigmented chorioretinal scar.3 Variable appearance of retinal toxoplasmosis lesions include large destructive lesions, punctate inner retinal lesions, or punctate outer retinal lesions, an atypical presentation.4 Punctate outer retinal toxoplasmosis (PORT) lesions are typically small, multifocal gray-white spots with little overlying vitreous reaction.4 This report describes an unusual case of PORT in a patient with multiple recurrences despite long-term prophylaxis.
Case Report
An 11-year-old female presented with decreased vision and floaters in both eyes. Medical history was unremarkable except occasional mild headaches. Pertinent family history included Guillain-Barre Syndrome in her father and recurrent Bartonella in her mother.
Ophthalmologic evaluation revealed best corrected visual acuity (BCVA) of 20/60 in the right eye, 20/25 in the left eye. Intraocular pressure, pupils, confrontational visual fields, and extraocular movements were normal in both eyes. Anterior segment exam was unremarkable. Dilated fundus exam, optical coherence tomography (OCT), ultra-widefield autofluorescence images, and fluorescein angiography demonstrated macular chorioretinal lesions (Figures 1A-B). Initial bloodwork included negative QuantiFERON Gold, negative fluorescent treponemal antibody absorbed test, and undetectable toxoplasmosis IgM. However, elevated toxoplasmosis IgG levels (311 IU/mL) combined with an abnormal retinal examination despite no significant anterior chamber inflammation led to a toxoplasmosis chorioretinitis diagnosis.
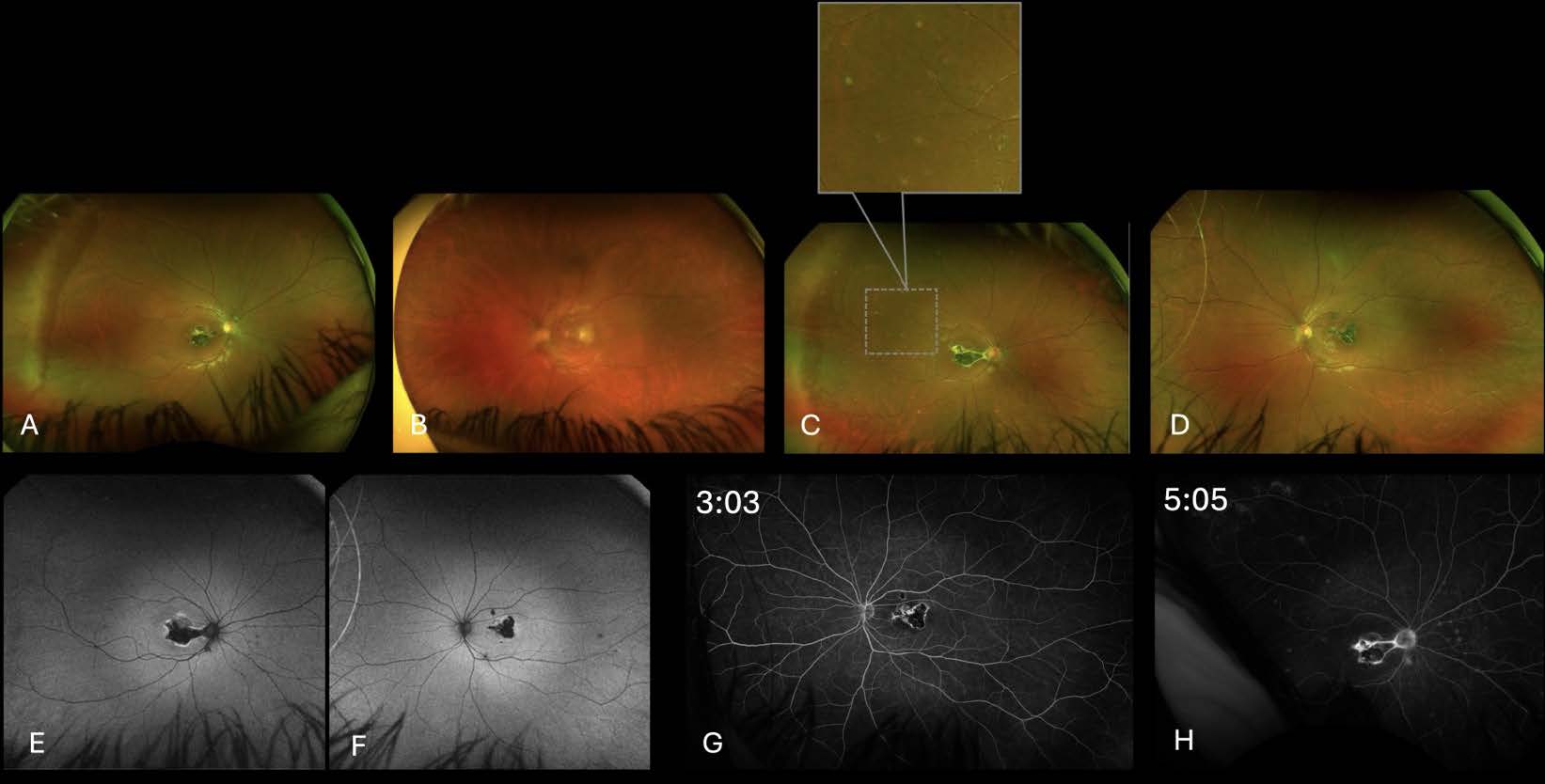
macular lesions. C. 33 months post-presentation right eye: larger macular scar with new focal hypopigmented
lesions. D. 33 months post-presentation left eye: evolution to macular scar. E. 33 months post-presentation right
eye: well demarcated complete hypoautofluorescnce in macula with hyperautofluorescent margins and
hypoautofluorescent punctate lesions in the mid-periphery (corresponding to the white punctate lesions in (C).
F. 33 months post-presentation left eye: well demarcated complete hypoautofluorescence in macula with
hyperautofluorescent margins. G. 33 months post-presentation left eye fluorescein angiography: blocked
fluorescence in macula with hyperfluorescent margins, no leakage. H. 33 months post-presentation right eye:
blocked fluorescence in macula with hyperfluorescent margins, no leakage.
Initial treatment included 1 mg/0.1 cc intravitreal clindamycin in the left eye and 500 mg oral azithromycin. Five days later, a 60 mg prednisone taper was initiated, followed by a several-week course of oral atovaquone 750 mg twice daily. Her symptoms improved and she began prophylactic once daily trimethoprimsulfamethoxazole (TMP-SMX), 160 mg/800 mg.
Five months post-presentation, recurrent toxoplasmosis developed in the right eye (Figure 2). Intravitreal clindamycin was administered, and TMP-SMX was increased to twice daily. After six weeks of improved symptoms, TMP-SMX was reverted to once daily. However, in subsequent months, she had two recurrences in the right eye. The first occurred while on TMP-SMX once daily, prompting increase to TMP-SMX BID and addition of atovaquone 1500 mg twice a day. The second occurred while on TMP-SMX twice a day but without atovaquone. Restarting atovaquone yielded quiescence for three months.
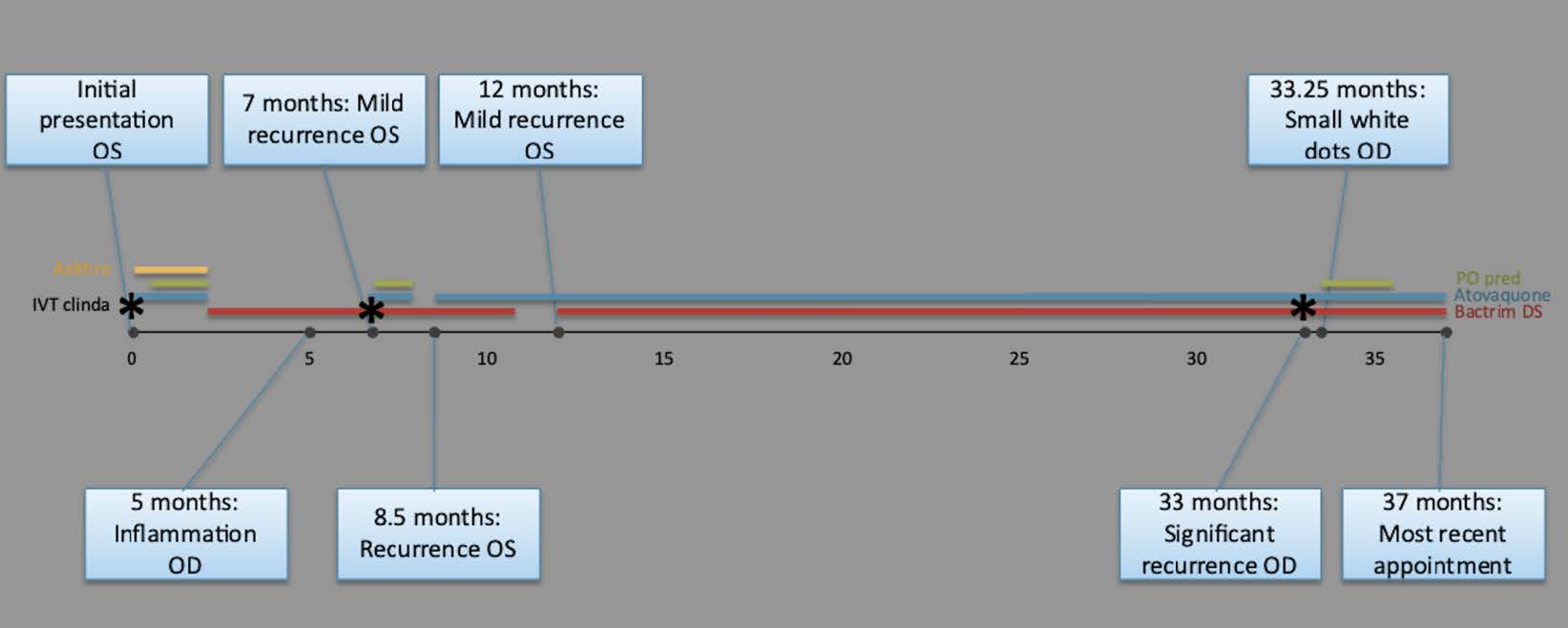
multiple recurrences despite treatment and prophylaxis.
Given prolonged stability, TMP-SMX was discontinued, though atovaquone was continued. Shortly after discontinuation, there was another recurrence in the left eye. TMP-SMX was restarted twice daily with subsequent quiescence for 21 months, until a recurrence developed in the right eye at 33 months postpresentation (Figures 1C-D). Intravitreal clindamycin yielded limited response, with the development of new mid-peripheral hypopigmented retinal lesions that did not leak on fluorescein angiography (Figures 1E-H) and were localized to the outer retina on OCT (Figure 3), consistent with PORT. A prednisone taper improved but did not normalize vision. She was evaluated by pediatric rheumatology for potential non-infectious components of her disease and found to have low-normal total globulins (2.0 g/dL) but no evidence of systemic rheumatologic pathology or other infections.
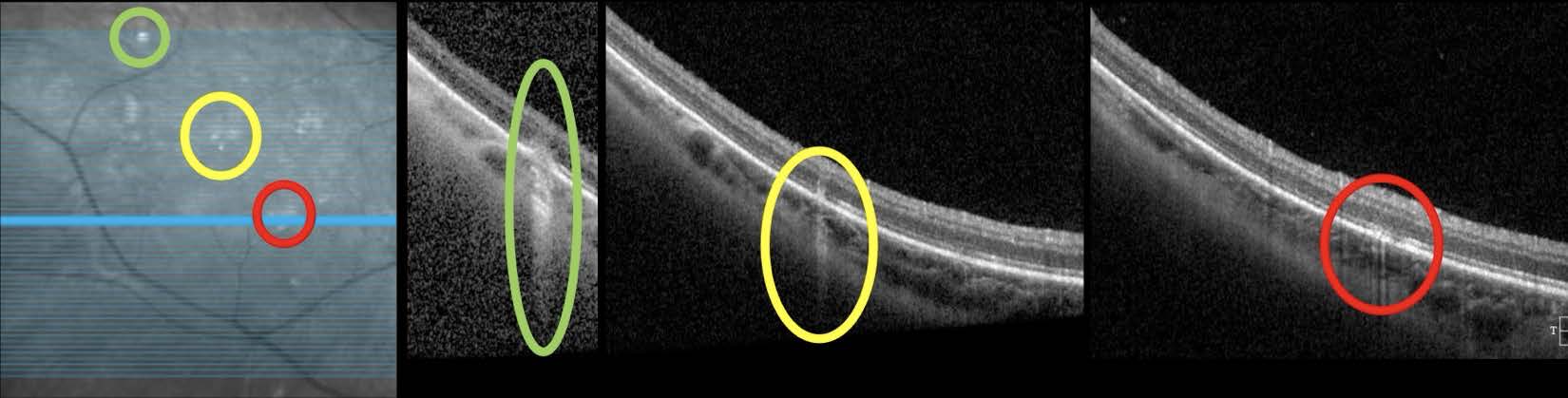
focal hyperreflective lesions involving the retinal pigment epithelium.
At 37 months post-presentation, visual acuity was 20/100 in the right eye, 20/25 in the left eye. Intraocular pressure was 20 mm Hg in both eyes. Confrontational visual fields and extraocular movement were normal in both eyes. An increased number of punctate white lesions were noted in the right eye. Fluorescein angiography showed staining inferior to the chorioretinal scar. Continued TMP-SMX twice a day was recommended.
Discussion
PORT lesions are an uncommon presentation of ocular toxoplasmosis and are characterized by small, multifocal lesions in the deep retinal layers and retinal pigment epithelium (RPE), with minimal vitreous inflammation compared to other subtypes.5 Unlike typical toxoplasmosis lesions, which affect all retinal layers, PORT lesions are confined to the outer nuclear layer. In our case, spectral-domain OCT imaging revealed these lesions as hyperreflective areas above the RPE, forming a subtle pitchfork sign. This sign, often associated with inflammatory choroidal neovascularization, could indicate active inflammation. Additionally, the PORT lesions demonstrated increased signal transmission, suggesting focal RPE loss, which correlated with their punctiform hypoautofluorescent appearance on fundus autofluorescence. These findings suggest that PORT lesions may be localized to the RPE interdigitation zone.
We present the first multimodal imaging report of PORT in a patient with multiple recurrences on long-term prophylaxis. Recurrence is not atypical after initial treatment; however, previous cases of recurrent PORT were reported in patients not on long-term prophylaxis.6 Additionally, we complement existing literature by providing multimodal imaging characteristics.
Systemic pyrimethamine, sulfadiazine, and corticosteroids is the most common initial treatment for ocular toxoplasmosis, but evidence suggests that intravitreal clindamycin and corticosteroid, as our patient received, is equally effective.3,7 It is known that treatment during active infection does not consistently prevent long-term recurrence. Recurrence occurs in up to half of cases, typically within a year after presentation.3,5,8 While our patient lacked several classic risk factors for recurrence, such as older age or clinically significant immunosuppression, some evidence suggests that macular involvement, as seen in this case, increases probability of recurrence.8 Furthermore, congenital toxoplasmosis is associated with risk of recurrence and cannot be ruled out in our patient, though postnatal infection is also likely.8
Prophylaxis for ocular toxoplasmosis is often recommended in immunocompromised patients, but its benefit for routine use is debated.9 Immunocompetent patients considered to be appropriate candidates for prophylaxis include those with multiple recurrences per year, or three within two years,9 as in this patient. Studies have established TMP-SMX prophylaxis as effective in preventing recurrences.10,11 The patient presented herein was taking long-term TMP-SMX at a higher dosing frequency than suggested by literature, thus expected to be adequate.
One recurrence did occur after briefly discontinuing TMP-SMX prophylaxis. However, two recurrences occurred while on TMP-SMX once daily: one after reduction from TMP-SMX twice a day, and one with no obvious trigger. Furthermore, two recurrences occurred while she was on TMP-SMX twice a day: one after stopping atovaquone and one with no clear precipitant. The low globulins may be a contributing factor for her recurrences. Systemic, though not ocular, toxoplasmosis has been reported in several patients with hypogammaglobulinemia, suggesting the importance of antibody-mediated immunity in overcoming toxoplasmosis.12 A case of central nervous system toxoplasmosis has also been reported in a child with hyper-IgM syndrome, presenting after treatment with prophylactic TMP-SMX for recurrent otitis media.13 The causes of our patient’s low-normal globulin level and its relationship with her recurrences are not fully understood. Future research to elucidate any potential benefits of earlier immune screening or specialized management of these patients may be of interest.
Conclusion
This report describes an atypical case of ocular toxoplasmosis, presenting as the rare punctate outer retinal subtype and recurring multiple times over several years despite adequate treatment and long-term prophylaxis. This patient’s lower globulins may have contributed to her presentation. Systemic toxoplasmosis has been reported in cases of hypogammaglobulinemia, but its link to ocular toxoplasmosis is not well established. Further study is warranted to investigate the association between globulinemia, PORT, and risk of recurrent toxoplasmosis despite treatment and prophylaxis.
References
1. Garweg J, Petersen E. Toxoplasmosis: Ocular Disease. UpToDate. Published May 4, 2024. Accessed July 5, 2024. https://www.uptodate.com/contents/toxoplasmosis-ocular-disease.
2. Atmaca L, Simsek T, Batioglu F. Clinical Features and Prognosis in Ocular Toxoplasmosis. Japanese Journal of Ophthalmology. 2004;48(4):386-391.
3. Gritz DC, Read RW, Khadamy J, et al. Toxoplasmosis. EyeWiki. Published February 25, 2024. Accessed July 5, 2024. https://eyewiki.org/Toxoplasmosis
4. Jabs D, Nguyen QD. Retina. 4th ed. Vol 2. St. Louis, MO: Mosby; 2006:1583-1595.
5. Kalogeropoulos D, Sakkas H, Mohammed B, et al. Ocular Toxoplasmosis: A Review of the Current Diagnostic and Therapeutic Approaches. Int Ophthalmol. 2022;42(2):295-32.
6. de Souza EC, Casella AMB. Clinical and Tomographic Features of Macular Punctate Outer Retinal Toxoplasmosis. Arch Ophthalmol. 2009;127(10):1390-1394.
7. Baharivand N, Mahdavifard A, Fouladi RF. Intravitreal Clindamycin Plus Dexamethasone Versus Classic Oral Therapy in Toxoplasmic Retinochoroiditis: A Prospective Randomized Clinical Trial. Int Ophthalmol. 2013;33(1):39-46.
8. Cifuentes-Gonz.lez C, Rojas-Carabali W, P.rez .O, et al. Risk Factors for Recurrences and Visual Impairment in Patients with Ocular Toxoplasmosis: A Systematic Review and Meta-Analysis. PLoS One. 2023;18(4).
9. Saffra NA, Seidman CJ, Weiss LM. Ocular Toxoplasmosis: Controversies in Primary and Secondary Prevention. J Neuroinfect Dis. 2013;4:235689.
10. Silveira C, Belfort R Jr, Muccioli C, et al. The Effect of Long-Term Intermittent Trimethoprim/Sulfamethoxazole Treatment on Recurrences of Toxoplasmic Retinochoroiditis. Am J Ophthalmol. 2002;134(1):41-46.
11. Fernandes Felix JP, Cavalcanti Lira RP, Grupenmacher AT, et al. Long-Term Results of Trimethoprim- Sulfamethoxazole Versus Placebo to Reduce the Risk of Recurrent Toxoplasma Gondii Retinochoroiditis. Am J Ophthalmol. 2020;213:195-202.
12. McDermott DH, Heusinkveld LE, Zein WM, et al. Case Report: Ocular Toxoplasmosis in a WHIM Syndrome Immunodeficiency Patient. F1000Research. 2019;8:2.
13. Leiva LE, Junprasert J, Hollenbaugh D, et al. Central Nervous System Toxoplasmosis with an Increased Proportion of Circulating γδ T Cells in a Patient with Hyper-IgM Syndrome. J Clin Immunol. 1998;18(4):283-290.
Statement of Ethics
This case report adheres to patient confidentiality and ethical principles in accordance with the guidelines of the
Declaration of Helsinki and relevant local regulations. A written informed consent was obtained from the
patient’s parents authorizing publication of this medical case and accompanying images.
Conflict of Interest Statement
R.M.: PYC Therapeutics - consultant; ProQR – consultant.
Funding
This work received no funding or grant support.
Authorship
We attest that all authors contributed significantly to the creation of this manuscript, each having fulfilled the
criteria as established by the ICMJE.